What is zentensivism, really?
I had the opportunity to give this presentation at The Hospitalist and Resuscitationist: Reloaded conference this year held by Philippe Rola (www.thinkingcriticalcare.com).

First and foremost, zentensivism is a holistic approach to the art of caring for the critically ill. It is minimalism, grounded in clinical mastery and risk tolerance, and motivated by humanism.
A reaction against this approach is “how do you just standby as clinical deterioration happens!?”
This is certainly not the case. As with usual care, a zentensivist rushes to the bedside of a crashing patient. The difference is in the care that happens thereafter. Zentensive care aims to get out of the way of the patient as soon as possible, removing interventions with the same speed.

To learn more about these ideas in depth, see our open access paper at ATS Scholar.
As previously mentioned, this type of medical care requires the clinician to have developed mastery forged by deliberate practice.
How can risk tolerance be developed? The first step is to challenge notions of what “abnormal” values can and cannot be tolerated.


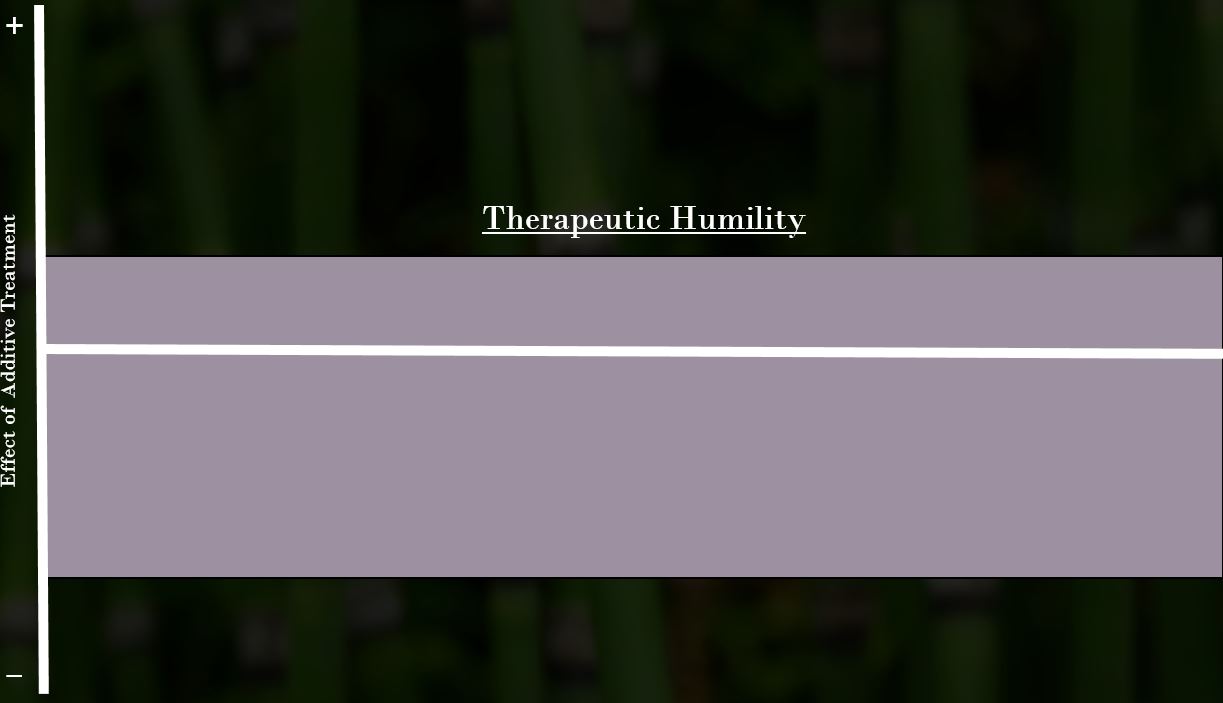
Additionally, we have to reconsider how effective our interventions really are. Many clinicians practice as if our interventions lead to large improvement with small, unmeasurable downsides.
The history of critical care does not support magic bullets. In fact, most interventions have a modest, measurable benefit and a large, sometimes unmeasurable downside. This idea is well-presented in Jacob Stegenga’s Medical Nihilism. This concept is shown graphically below. The gray graph is a better representation of reality, and incorporates necessary therapeutic humility.

Most importantly, preserving humanism is an ethical imperative in the care of the critically ill.

Where am I meeting this patient in their (acute and chronic) disease trajectory, what are the viable treatment options, and do they make sense for this person and their goals? Zentensivism has its roots in this question.
While the care is “minimalist”, the attention to the patient as a person and their clinical data is even higher. We refer to this as minimally invasive, maximally attentive care. And it is more work than usual care!

Minimalism requires carefully choosing not to make knee-jerk interventions, close monitoring, and intentional, out-loud metacognition for the patient and care team to understand the reasoning behind the philosophy.
We feel that this is the way to practice critical care medicine.
